Search the Community
Showing results for tags 'national certification'.
Found 8 results
-
 View this email in your browser Wandering Residents In residential aged care facilities there are many factors that may influence residents to wander. These commonly include: Inactivity/boredom – lack of activity may lead the person to wander around looking for something to do. In some instances wandering dissipates loneliness and the behavior in and of itself, is often a substitute for lack of social interaction. In contradiction, wandering surprisingly may also be a response to overstimulation and overwhelming situations. Fear, agitation, and confusion commonly lead to “dementia” wandering outdoors or in public environments. Some emotional cues that can cause wandering include: increased levels of stress or fear. Residents with “dementia” who wander are moving about in ways that may appear aimless but often have purpose. People may wander in response to an unmet basic need like human contact, hunger, or thirst; a noisy or confusing environment; or because they are experiencing some type of distress, like pain or the need to use the toilet. Wandering can be helpful or dangerous, depending on the situation. The Balancing Act It’s a balancing act for sure but it is important to look beyond the words or behaviors to discover the feelings that the resident might earnestly be trying to express. Strong emotions may also be caused by unmet needs. Staff must implement the process of deduction to work out what needs are not being addressed and meet the resident “where they are” when possible. Residents may wander for any number of reasons: Physical needs Psychological and social needs Cognitive needs Non-goal-directed wandering requires a response in a manner that addresses both safety issues and an evaluation to identify root causes to the degree possible. Moving about the facility aimlessly may indicate that the resident is frustrated, anxious, bored, hungry, or depressed. Although people who wander may gain social contact, exercise, and stimulation, the resident may consequently become lost or exhausted. Hence, they may become overwhelmed and over tired, which predictably causes sudden outwardly hasty behaviors such as wandering or higher probability of injuries to self and/or others. Person-Centered Care for Wandering Behavior Simply stated, some basic principles for people with dementia stems from understanding and supporting the residents’ rights. To be sure, the onset of dementia does not preclude inherently due personal rights. Understand that the individual beyond the “dementia” is becoming increasingly hidden rather than lost. This means that he/she is still there, and it’s your mission to reclaim the essence of the individual that once was and bring them out of hiding. Those who were highly sociable and had an active lifestyle prior to having mental decline are most likely to wander. The use of certain antipsychotic medications can cause side effects that increase the desire to wander and be in perpetual motion. Sedating medications can also increase the risk for wandering due to confusion. Other causes of wandering include the following: Memory deficits Poor vision Disorientation Language deficits Searching for security Searching to fulfill an unmet need such as to relieve hunger, thirst, pain, constipation, and the need to urinate Searching for a loved one Boredom Person centered care plans must consequently demonstrate this principle. Here are some examples of appropriate goals: Personalize the resident’s surroundings. Interpret behavior from the resident’s viewpoint. Acknowledge and validate the resident’s feelings. Involve the resident with dementia in decision-making. Create target goals for the resident to achieve based on resident history and his/her skills that have not yet been lost. Focus on the journey- not the results. Evaluate the Behavior Physical Needs: Does the resident need to use the bathroom? Is the behavior due to medication side affects? Is the resident: Hungry, thirsty, or generally uncomfortable? Searching for a place that is warmer or cooker, darker or lighter? Looking for a place that is more familiar (does the resident have familiar belongings in his/her room)? Responding to physical illness, e.g., dehydration, infection, congestive heart failure, etc.? Psychological and Social Needs: Is the resident: Restless or agitated and trying to relieve anxiety? Bored, lonely, or seeking company? Following a previously familiar imprinted routine: acting out movement to and from the bus stop to pick up the children – going to work? Cognitive Needs: Is the resident: Disoriented or lost? Disoriented due to medication side affects Overstimulated or understimulated? For the resident, wandering may be positive if it fulfills a need for exercise, sensory stimulation, or purposeful behavior. Many nursing homes provide a safe environment on a locked unit for this reason. The negative side of wandering is it may lead to falls, excess fatigue, anxiety, accidental exposure to certain chemicals, altercations with other residents and unintended wandering outdoors where more danger may be waiting to cause harm. Make it your mission to find the balance in the day and life of your resident by looking beyond the words or behaviors to discover the feelings that the resident might earnestly be trying to express. Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2021 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2810 US HWY 190 W #100-A9 Livingston, Texas 77351
View this email in your browser Wandering Residents In residential aged care facilities there are many factors that may influence residents to wander. These commonly include: Inactivity/boredom – lack of activity may lead the person to wander around looking for something to do. In some instances wandering dissipates loneliness and the behavior in and of itself, is often a substitute for lack of social interaction. In contradiction, wandering surprisingly may also be a response to overstimulation and overwhelming situations. Fear, agitation, and confusion commonly lead to “dementia” wandering outdoors or in public environments. Some emotional cues that can cause wandering include: increased levels of stress or fear. Residents with “dementia” who wander are moving about in ways that may appear aimless but often have purpose. People may wander in response to an unmet basic need like human contact, hunger, or thirst; a noisy or confusing environment; or because they are experiencing some type of distress, like pain or the need to use the toilet. Wandering can be helpful or dangerous, depending on the situation. The Balancing Act It’s a balancing act for sure but it is important to look beyond the words or behaviors to discover the feelings that the resident might earnestly be trying to express. Strong emotions may also be caused by unmet needs. Staff must implement the process of deduction to work out what needs are not being addressed and meet the resident “where they are” when possible. Residents may wander for any number of reasons: Physical needs Psychological and social needs Cognitive needs Non-goal-directed wandering requires a response in a manner that addresses both safety issues and an evaluation to identify root causes to the degree possible. Moving about the facility aimlessly may indicate that the resident is frustrated, anxious, bored, hungry, or depressed. Although people who wander may gain social contact, exercise, and stimulation, the resident may consequently become lost or exhausted. Hence, they may become overwhelmed and over tired, which predictably causes sudden outwardly hasty behaviors such as wandering or higher probability of injuries to self and/or others. Person-Centered Care for Wandering Behavior Simply stated, some basic principles for people with dementia stems from understanding and supporting the residents’ rights. To be sure, the onset of dementia does not preclude inherently due personal rights. Understand that the individual beyond the “dementia” is becoming increasingly hidden rather than lost. This means that he/she is still there, and it’s your mission to reclaim the essence of the individual that once was and bring them out of hiding. Those who were highly sociable and had an active lifestyle prior to having mental decline are most likely to wander. The use of certain antipsychotic medications can cause side effects that increase the desire to wander and be in perpetual motion. Sedating medications can also increase the risk for wandering due to confusion. Other causes of wandering include the following: Memory deficits Poor vision Disorientation Language deficits Searching for security Searching to fulfill an unmet need such as to relieve hunger, thirst, pain, constipation, and the need to urinate Searching for a loved one Boredom Person centered care plans must consequently demonstrate this principle. Here are some examples of appropriate goals: Personalize the resident’s surroundings. Interpret behavior from the resident’s viewpoint. Acknowledge and validate the resident’s feelings. Involve the resident with dementia in decision-making. Create target goals for the resident to achieve based on resident history and his/her skills that have not yet been lost. Focus on the journey- not the results. Evaluate the Behavior Physical Needs: Does the resident need to use the bathroom? Is the behavior due to medication side affects? Is the resident: Hungry, thirsty, or generally uncomfortable? Searching for a place that is warmer or cooker, darker or lighter? Looking for a place that is more familiar (does the resident have familiar belongings in his/her room)? Responding to physical illness, e.g., dehydration, infection, congestive heart failure, etc.? Psychological and Social Needs: Is the resident: Restless or agitated and trying to relieve anxiety? Bored, lonely, or seeking company? Following a previously familiar imprinted routine: acting out movement to and from the bus stop to pick up the children – going to work? Cognitive Needs: Is the resident: Disoriented or lost? Disoriented due to medication side affects Overstimulated or understimulated? For the resident, wandering may be positive if it fulfills a need for exercise, sensory stimulation, or purposeful behavior. Many nursing homes provide a safe environment on a locked unit for this reason. The negative side of wandering is it may lead to falls, excess fatigue, anxiety, accidental exposure to certain chemicals, altercations with other residents and unintended wandering outdoors where more danger may be waiting to cause harm. Make it your mission to find the balance in the day and life of your resident by looking beyond the words or behaviors to discover the feelings that the resident might earnestly be trying to express. Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2021 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2810 US HWY 190 W #100-A9 Livingston, Texas 77351



-
 Dealing With Elderly Anger Outbursts & Hostility As healthcare professionals many of us if not all has encountered a resident that is not having a good day. It is not all that unexpected however, in our line of work to experience outbursts and hostility mood swings. They may result from dissatisfaction, poor health, stress, pain, and a loss of dignity can easily lead to surprising and potentially harmful behaviors cause undue emotional hardships on both staff and residents alike. These scenarios are emotionally stressful for all parties and may need a considerable amount of energy, patience and empathy, to redirect. Research studies report that “mood disorders are frequent in old age and their prevalence is increasing with population aging.” https://companionsforseniors.com/2019/04/mood-swings-elderly-seniors/#:~:text=Another%20prominent%20research%20study%20notes,therapy%2C%20or%20a%20medication%20regimen Getting older can magnify our unique character traits, often in undesirable ways. Someone who was crabby in their younger years may be prone to full-on bouts of range in the aging years. Unfortunately, fellow residents and our professional staff members often are the target of these outbursts, and although in many cases it may seem at times as though there was no apparent clinical “trigger” such as a diagnosis of Alzheimer’s or prolonged chronic pain that may be attributed to the root cause; these behaviors are non-the-less and often enough, the most challenging to overcome. Know Your Resident That said, there are tried and true strategies and techniques that you will need to master to turn around a bad day into a pleasant (uneventful) good day. Below you can learn about several well described options that offer alternatives to reduce the tension and redirect even the most “crankiest of crannies” and help preserve your own mental wellbeing in the process. Simply stated, one of the most effective “tried and true” strategies is to know your resident. A thorough and comprehensive understanding of the elements that have potential to trigger your resident long before it leads down that unwanted behavior rabbit hole will always save the day. Clearly, this is not going to happen as quickly as one would hope for but with consistent observation/evaluation and comprehensive documentation such as Behavior Logs, will greatly identify the root cause of the problem be implemented in the resident Care Plan as Behavioral Interventions. Most importantly, be mindful to ensure that every staff member (all shifts and disciplines) are aware of these triggers. Communication and consistent unilateral Interdisciplinary staff support are major factors to this success story. Note that is can take up to “TWO” weeks for a resident to give up unwanted behavior because the behavior has become a coping pattern and is all the resident knows to find comfort. How to Handle Elderly Anger Outbursts The first step to dealing with these problems is to understand that these negative emotions are not personal. Pain and disease has an undeniably strong potential to cause very inappropriate behavior. The best strategy when dealing with difficult elders has a great deal to do with (Four C’s) - communication, clarity, consistency and compassion. Be mindful that optimum communication breakdowns between staff and resident may be further compounded by receptive and expressive resident impairments. Be consistent, repetition will enforce the concept of desired change. Cursing and Abusive Language Verbal abuse and harsh language can be an even more complicated story. Profanities that are “out-of-character” are often the result of Alzheimer’s disease, which can make it particularly difficult to manage. While there’s no cure for some conditions that present cursing and abusive language, mitigating the behavior can often be achieved by using distractions in the form of redirection. For example, divert your residents swearing bout by introducing another scenario that you are certain will be well received as more desirable and enticing by your resident. Example: “Mary I need your help today to make your favorite dessert – let’s go to the kitchen to get the ingredients ready.” Paranoia and Hallucinations Residents may believe that others want to cause them personal harm. In some instances the clinical team has already noted that the resident suffers from paranoia or hallucinations or another disorder that is a known root cause. It is not uncommon for paranoid behavior to be associated with a diagnosed disease such as Alzheimer’s disease but there are other illnesses that will also lead to paranoia. In these cases, the best solution to the problem of paranoid behavior is to try and use relaxation and validation techniques. Additionally, this may need to be combined with medication management. You generally won’t be able to convince someone what they’re experiencing is unreal, and doing so may increase the residents’ frustration or anger. Note that it is reasonable to go along with the residents’ allusion when the experience in of itself is clearly pleasant and does not have the potential to cause harm to self or others. Attentive patience and consistent caring oversight has everything to do with your residents’ success story and yours. “Perseverance is not a long race; it is many short races one after the other.” -Walter Elliot https://www.agingcare.com/articles/how-to-handle-an-elderly-parents-bad-behavior-138673.htm https://www.griswoldhomecare.com/blog/2015/july/dealing-with-elderly-anger-outbursts-hostility/ Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2022 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2810 US HWY 190 W Ste 100-A9 Livingston, Texas 77351
Dealing With Elderly Anger Outbursts & Hostility As healthcare professionals many of us if not all has encountered a resident that is not having a good day. It is not all that unexpected however, in our line of work to experience outbursts and hostility mood swings. They may result from dissatisfaction, poor health, stress, pain, and a loss of dignity can easily lead to surprising and potentially harmful behaviors cause undue emotional hardships on both staff and residents alike. These scenarios are emotionally stressful for all parties and may need a considerable amount of energy, patience and empathy, to redirect. Research studies report that “mood disorders are frequent in old age and their prevalence is increasing with population aging.” https://companionsforseniors.com/2019/04/mood-swings-elderly-seniors/#:~:text=Another%20prominent%20research%20study%20notes,therapy%2C%20or%20a%20medication%20regimen Getting older can magnify our unique character traits, often in undesirable ways. Someone who was crabby in their younger years may be prone to full-on bouts of range in the aging years. Unfortunately, fellow residents and our professional staff members often are the target of these outbursts, and although in many cases it may seem at times as though there was no apparent clinical “trigger” such as a diagnosis of Alzheimer’s or prolonged chronic pain that may be attributed to the root cause; these behaviors are non-the-less and often enough, the most challenging to overcome. Know Your Resident That said, there are tried and true strategies and techniques that you will need to master to turn around a bad day into a pleasant (uneventful) good day. Below you can learn about several well described options that offer alternatives to reduce the tension and redirect even the most “crankiest of crannies” and help preserve your own mental wellbeing in the process. Simply stated, one of the most effective “tried and true” strategies is to know your resident. A thorough and comprehensive understanding of the elements that have potential to trigger your resident long before it leads down that unwanted behavior rabbit hole will always save the day. Clearly, this is not going to happen as quickly as one would hope for but with consistent observation/evaluation and comprehensive documentation such as Behavior Logs, will greatly identify the root cause of the problem be implemented in the resident Care Plan as Behavioral Interventions. Most importantly, be mindful to ensure that every staff member (all shifts and disciplines) are aware of these triggers. Communication and consistent unilateral Interdisciplinary staff support are major factors to this success story. Note that is can take up to “TWO” weeks for a resident to give up unwanted behavior because the behavior has become a coping pattern and is all the resident knows to find comfort. How to Handle Elderly Anger Outbursts The first step to dealing with these problems is to understand that these negative emotions are not personal. Pain and disease has an undeniably strong potential to cause very inappropriate behavior. The best strategy when dealing with difficult elders has a great deal to do with (Four C’s) - communication, clarity, consistency and compassion. Be mindful that optimum communication breakdowns between staff and resident may be further compounded by receptive and expressive resident impairments. Be consistent, repetition will enforce the concept of desired change. Cursing and Abusive Language Verbal abuse and harsh language can be an even more complicated story. Profanities that are “out-of-character” are often the result of Alzheimer’s disease, which can make it particularly difficult to manage. While there’s no cure for some conditions that present cursing and abusive language, mitigating the behavior can often be achieved by using distractions in the form of redirection. For example, divert your residents swearing bout by introducing another scenario that you are certain will be well received as more desirable and enticing by your resident. Example: “Mary I need your help today to make your favorite dessert – let’s go to the kitchen to get the ingredients ready.” Paranoia and Hallucinations Residents may believe that others want to cause them personal harm. In some instances the clinical team has already noted that the resident suffers from paranoia or hallucinations or another disorder that is a known root cause. It is not uncommon for paranoid behavior to be associated with a diagnosed disease such as Alzheimer’s disease but there are other illnesses that will also lead to paranoia. In these cases, the best solution to the problem of paranoid behavior is to try and use relaxation and validation techniques. Additionally, this may need to be combined with medication management. You generally won’t be able to convince someone what they’re experiencing is unreal, and doing so may increase the residents’ frustration or anger. Note that it is reasonable to go along with the residents’ allusion when the experience in of itself is clearly pleasant and does not have the potential to cause harm to self or others. Attentive patience and consistent caring oversight has everything to do with your residents’ success story and yours. “Perseverance is not a long race; it is many short races one after the other.” -Walter Elliot https://www.agingcare.com/articles/how-to-handle-an-elderly-parents-bad-behavior-138673.htm https://www.griswoldhomecare.com/blog/2015/july/dealing-with-elderly-anger-outbursts-hostility/ Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2022 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2810 US HWY 190 W Ste 100-A9 Livingston, Texas 77351 -
Apncc.org
-
Do You Need APNCC.org PreApproved CEU's for Your National Certification Requirements View this email in your browser A fun night out to the movies no longer needs to include the 'out' part. Watching movies from the comfort of where you live has never been easier and it is an activity your residents will love. We don't want to just turn a movie on and walk off, though. Let's make it an event! A bunch of them in fact. I am talking about a Movie Month! Plan one movie night per week and go all out for it. Hand out tickets, serve popcorn, soda, candy, etc. Decorate the movie area so it feels like like leaving home. You can add curtains to each side of the TV, setup a ticket taking area, and hang movie posters. Get people hyped up for movie night all week by keeping the movie a secret. Each day make an announcement with one piece of trivia from the movie and let them all guess throughout the week, with the answer being revealed on the screen. Keep residents involved in the movie selection by having them all submit their choice and you can select 4 common ones from there. To maintain interest you could also serve a different treat each movie night. For example, coke floats, banana splits, ice cream cones, and sundaes. Below are some ideas to get your planning going! I found this free resource from familystrong.blogspot.com and created a printable page with a variety of tickets for you to print out and use. For best results print on card stock. Movie Ticket Printable Reveal Answers "The secret to 'stay crispy' popcorn is Clarified Butter." Once you have your clarified butter ready, make your popcorn using it and as a topping. The optional coloring mentioned is a mixture of turmeric and saffron. Click on either picture to view the full recipe. Get Full Recipe HERE Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2021 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2810 US HWY 190 W #100-A9 Livingston, Texas 77351 Want to change how you receive these emails? You can update your preferences or unsubscribe from this list.


-
This recognition will take place May 9-15 and will honor the collaborative commitment of skilled nursing care facilities and their staff in providing compassionate care to their residents during these unprecedented times. Over the past year, despite the challenges of the current pandemic, skilled care centers and their staff have shown an incredible and steadfast commitment to providing quality care and ensuring the safety of their residents. This recognition does not come as a surprise given the daunting challenges that our front line “essential workers” have had to overcome to ensure the safety and well being of our residents. The week will focus on the collective efforts and the amazing strength and dedication of those who worked tirelessly each and every day to care for and protect the frail, elderly, and disabled adults in long term care. With each new season comes new beginnings, and together we will get to a place and time of healing. Why is it Important to Recognize Milestones Nevertheless, celebrating milestones along the path towards our goals is a crucial component of engagement. It helps honor the hard work folks are putting in, recognizing achieved goals, and simply creates a more positive environment. The intent to offer time to recognize these areas sprinkles coveted “positivity” throughout the facility for both residents and staff members. Milestones, whether personal or work-related, become inspiring memories that are needed to renew our energy supply and shouldn't go unrecognized. Celebrating achievements is a way for us to see how far we've come and can serve as our motivation should another challenge present itself. When recognition brings attention to efforts having a direct impact on the success of a company, it motivates staff and contributes to a sense of united celebratory reward that values the staff and honors resident well being. It also contributes greatly to meaningful organizational purpose. Programming Ideas Established by the American Health Care Association (AHCA) in 1967, NSNCW, formerly known as National Nursing Home Week, recognizes the essential role of skilled nursing care centers in caring for America’s frail, elderly, and disabled. This coming May, celebrate all members of your community and participate on social media using the hashtag #NSNCW. Below is a list of general activity ideas taken from the American Health Care Association/ National Center for Assisted Living: NOTE: At the time of publishing, care centers were following social distancing and other restrictions due to COVID-19. Please be sure to plan your activities through an infection prevention and control lens and modify them based on the latest guidelines as needed. Celebrate Together coordinates interactive games and raffles. Decorate and provide food to staff in celebration and appreciation of their efforts. If safe and guidelines allow, invite family members to share a meal with residents. Plan a themed dress-up day or a dance contest and offer prizes. Create Together Engage residents in creative art projects focused on the theme of the four seasons and togetherness. Coordinate a project that allows everyone to participate such as a fingerprint or button tree. Display all artwork in a “gallery” and invite staff members on a “gallery walk”. Reaching Out Together Find ways to connect to the wider community. Ask loved ones, members of the community, and/or local school groups to send feel-good notes, drawings, or video messages for residents and staff. Work with residents to create signs and messages of their own to share with loved ones. Enjoy Music Together Plan a concert or talent show and invite residents and staff with musical talents to share their gifts by playing or singing. Create personalized playlists for residents with dementia through the Music & Memory program. Music is the universal language and a great way to foster connections. https://www.ahcancal.org/Education-Events/Documents/NSNCW/NSNCW_2021_FINAL.pdf?csf=1&e=8EmyYh Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org Enroll Now Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2021 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2010 US HWY 190 W Ste 120 Livingston, Texas 77351
-
The time we have all been waiting for has finally arrived…..I Love Lucy Day is near. October 15th is a time for Lucy lovers everywhere to come together and show their appreciation for the original queen of comedy, the glass ceiling shattering, the studio owning, the great, the one and the only Lucille Ball! This Activity Corner is dedicated to all things Lucy. Prepare events to accompany an I Love Lucy Watch-A-Thon at your facility. Each activity suggestion can be incorporated throughout the day. If you really wanted to sell it, you could wear a Lucy costume. It will be Halloween time after all. 1" Bottlecap Template Printable Crossword Theme Music Which of your residents are Lucy’s #1 Fan? Many of us have seen the episodes so many times we could recite the script word for word. couldn’t we? Below is the actual script from Season 1, Episode 1 - The Girls Want to Go to the Nightclub. You use this script in a couple of ways. You can either print it out and mark out some of the lines and hand copies out to your residents. Allow them time to fill in what lines they think are missing. The one with the most correct/closest answers wins! Or you could re-enact a scene over the loudspeaker radio show style, in honor of I Love Lucy’s roots. Below is the beginning of the script. Click the button below to see the full script. (I Love Lucy theme music plays) (theme song ending) Here, you missed something on this one. That's the design. It is? Sure, can't you see? Flowers against a background of...gravy. I've been meaning to talk to you about Monday night. We want you and Ricky to help us celebrate. It's our wedding anniversary. Oh, yours and Fred's? No, me and Gregory Peck. We've been married for 18 years and I vowed that at least once before I died, Fred was going to take me to a nightclub on our wedding anniversary. Well, that sounds reasonable. Now, this is my plan. We'll go in there and I'll say: "I know what let's do next Monday night. Let's go to a nightclub." And you second the motion. Then Ricky will bound to his feet and say "That's great." Then Fred will have to take me because if... Ricky bounds to his feet and says, "That's great"? Right. Wrong. Ricky hates nightclubs. But he works in one. Your life should be just one gay round of nightclubs. Yeah, that's what I thought when I married a bandleader, but ever since we said "I do", there are so many things we don't. Full Script Fill your cart up with Cuban specialties in honor of the main fella in Lucy’s life, Ricky Ricardo. These appetizers are simple and easy to serve in disposable containers. Serve along with Mariquitas, plantain chips, a Cuban tradition. Cuban Sandwich On A Stick Appetizer Total Time: 10 minutes Servings: 24 Author: Katie Crenshaw Ingredients 6 slices of ham 24 swiss cheese cubes 24 mini dill pickles or cornichons 2 tbs whole grain mustard 24 to toothpicks Get Full Recipe HERE Circa 1950's Second Honeymoon Enroll Now Over a 100 Students graduating this session. Come Join In., It Starts Tomorrow. NAPT Activity Training Course for NAAPCC National Association of Activity Professionals Credentialing Center is the Most Highly Respected Certifying Body in the United States. Members in Good Standing with the NCCA "National Commission for Certifying Agencies" since 2011 View the requirements , NAAPCC Certification Standards Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2020 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2010 US HWY 190 W Ste 120 Livingston, Texas 77351
-
From NAAPCC NAAPCC DOES MEET FEDERAL TAG #658 NOTICE TO ALL ACTIVITY PROFESSIONALS Contrary to a notice posted 7-1-20 sent out by another organization, NAAPCC DOES meet federal Tag #658 as it is written and will post the full regulation on our website. You can also find it at the CMS website. The regulation states that CMS accepts the standards of ANY accrediting body or State Association, not just NAAP. The Training courses accepted under F Tag 680 only have to meet State approval. They DO NOT need to meet NAAP's approval or be accepted by them. NAAP is a membership organization for Activity Professionals, just as there are other organizations for Activity Professionals. No organization has the authority to approve someone else's work or decide what CMS will accept, nor is that stated anywhere in the regulations. NAAP has their own education and it would be a conflict of interest for them to approve or not approve other courses. The Creators of the NAPT course have no obligation to hand it over to anyone else for review. While NAAP is mentioned by name in one section, along with several other entities in F Tag 658, it is not an exclusive recognition, and following NAAP's name is the word "etc", meaning other organization standards are also recognized, including State Associations and Accrediting bodies, which does in fact include NAAPCC. Please be assured the information released is inaccurate. CMS has been recognizing and accepting NAAPCC certifications since 2011 and they also accept any State approved course per F Tag 680. If NAAP chooses to not promote other courses or certifications, that is their right, but they have no authority to decide what meets regulations. Please read below! The Highlighted sections dictate how NAAPCC meets the regulation. NAAPCC Standards are posted on the website. Recommended resources for manuals, etc., are also located on our website. o F658 GUIDANCE §483.21(b)(3)(i) “Professional standards of quality” means that care and services are provided according to accepted standards of clinical practice. Standards may apply to care provided by a particular clinical discipline or in a specific clinical situation or setting. Standards regarding quality care practices may be published by a professional organization, licensing board, accreditation body or other regulatory agency. Recommended practices to achieve desired resident outcomes may also be found in clinical literature. Possible reference sources for standards of practice include: • Current manuals or textbooks on nursing, social work, physical therapy, etc. • Standards published by professional organizations such as the American Dietetic Association, American Medical Association, American Medical Directors Association, American Nurses Association, National Association of Activity Professionals, National Association of Social Work, etc. • Clinical practice guidelines published by the Agency for Healthcare Research and Quality. • Current professional journal articles. Our credentials are recognized by CMS under F tags 658 and 680. If you have any questions or concerns please call the office at 303-317-5682 or email us at naapcc.office@gmail.com. We're here to assist you in any way we can. NAAPCC NAAP Credentialing Center 17840 Weymouth Ave, Parker CO 80134 United States You received this email because you signed up on our website or made a purchase from us. Unsubscribe
-
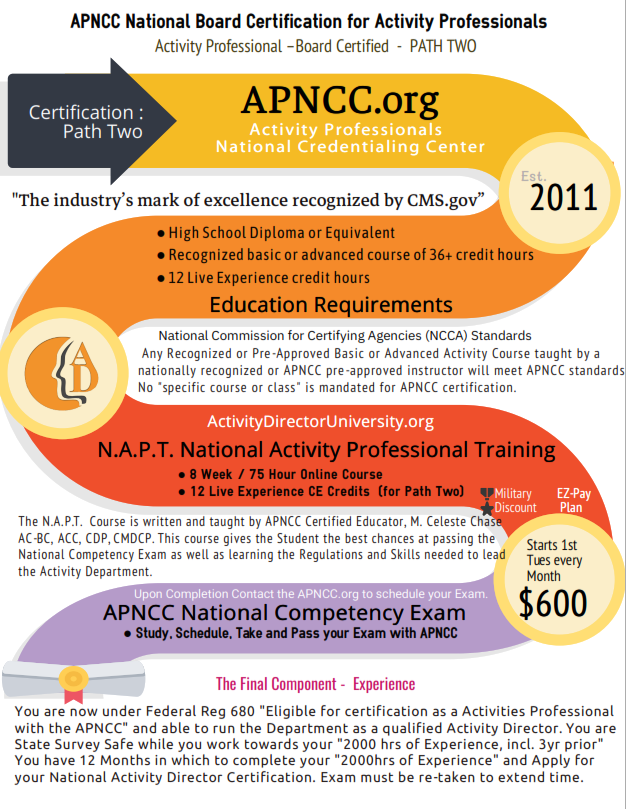
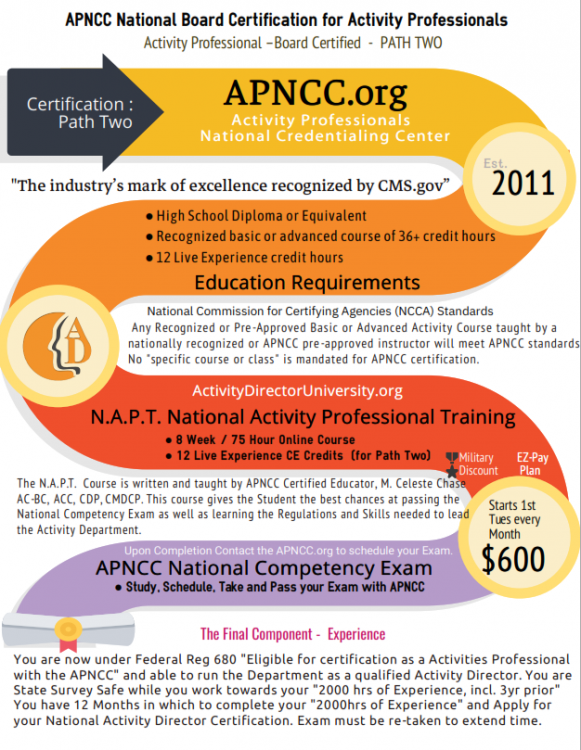
Adaptive Strategies and Techniques Without a doubt, it is important to identify whether the residents have conditions and/or issues for which staff should implement adaptations to allow the resident to fully enjoy the experience. The following is a simplified reference guide examples of specific conditions and appropriate adaptations: Visual impairments: higher levels of lighting without glare; magnifying glasses, light-filtering lenses, telescopic glasses; use of “clock method” to describe where items are located; description of sizes, shapes, colors; large print items including playing cards, newsprint, books; audio books; Hearing impairments: small group activities; placement of resident near speaker/activity leader; use of amplifiers or headphones; decreased background noise; written instructions; use of gestures or sign language to enhance verbal communication; adapted TV (closed captioning, magnified screen, earphones); Physical limitations: the use of adaptive equipment, proper seating and positioning, placement of supplies and materials (based on clinical/nursing or physical therapy referral as appropriate) to enhance: Visual interaction and to compensate for loss of visual field (hemianopsia); Upper extremity function and range of motion (reach); Hand dexterity (e.g., adapted size of items such as larger handles for cooking and woodworking equipment, built-up paintbrush handles, large needles for crocheting); The ability to manipulate an item based upon the item’s weight, such as lighter weight for residents with muscle weakness; Use of only one hand: holders for kitchen items, magazines/books, playing cards; items (e.g., artwork, bingo card, nail file) taped to the table; c-clamp or suction vise to hold wood for sanding; Cognitive impairment: task segmentation and simplification; programs using retained long-term memory, rather than short-term memory; length of activities based on attention span; settings that recreate past experiences or increase/decrease stimulation; smaller groups without interruption; one-to-one activities; NOTE: The length, duration, and content of specific one-to-one activities are determined by the specific needs of the individual resident, such as several short interventions (rather than a few longer activities) if someone has extremely low tolerance or if there are behavioral issues. Examples of one-to-one activities may include any of the following: Sensory stimulation or cognitive therapy (e.g., touch/visual/auditory stimulation, reminiscence, or validation therapy) such as special stimulus rooms or equipment; alerting/upbeat music and using alerting aromas or providing fabrics or other materials of varying textures; Social engagement (e.g., directed conversation, initiating a resident to resident conversation, pleasure walk or coffee visit); Spiritual support, nurturing (e.g., daily devotion, Bible reading, or prayer with or for resident per religious requests/desires); Creative, task-oriented activities (e.g., music or pet activities/therapy, letter writing, word puzzles); Support of self-directed activity (e.g., delivering of library books, craft material to rooms, setting up talking book service). Language barrier: translation tools; translators; or publications and/or audio/video materials in the resident’s language; Terminally ill: life review; quality time with chosen relatives, friends, staff, and/or other residents; spiritual support; touch; massage; music; and/or reading to the resident; NOTE: Some residents may prefer to spend their time alone and introspectively. Their refusal of activities does not necessarily constitute noncompliance. Pain management: spiritual support, relaxation programs, music, massage, aromatherapy, pet therapy/pet visits, and/or touch; Solitary preferences/own room or is unable to leave room: in-room visits by staff/other residents/volunteers with similar interests/hobbies; touch and sensory activities such as massage or aromatherapy; access to art/craft materials, cards, games, reading materials; access to technology of interest (computer, DVD, hand held video games, preferred radio programs/stations, audio books); and/or visits from spiritual counselors; Altering sleep patterns: activities are available during awake time. Some facilities use a variety of options when activities staff are not available for a particular resident: nursing staff reads a newspaper with resident; dietary staff makes finger foods available; CNA works puzzle with the resident; maintenance staff take the resident on night rounds; and/or early morning delivery of coffee/juice to residents; Miscellaneous; Short-stay resident: “a la carte activities” are available, such as books, magazines, cards, word puzzles, newspapers, CDs, movies, and handheld games; interesting/contemporary group activities are offered, such as dominoes, bridge, Pinochle, poker, video games, movies, and travelogues; and/or individual activities designed to match the goals of therapy, such as jigsaw puzzles to enhance fine motor skills; Younger resident: individual and group music offerings that fit the resident’s taste and era; magazines, books and movies that fit the resident’s taste and era; computer and Internet access; and/or contemporary group activities, such as video games, and the opportunity to play musical instruments, card and board games, and sports Diverse ethnic or cultural backgrounds: special events that include meals, decorations, celebrations, or music; visits from spiritual leaders and other individuals of the same ethnic background; printed materials (newspapers, magazines) about the resident’s culture; and/or opportunities for the resident and family to share information about their culture with other residents, families, and staff. Have a topic request or question for Celeste? Send them over to celestechase@activitydirector.org The NAPT- National Activity Professionals Training Course is written and taught by Celeste Chase, AC-BC, ACC, CDP, DMDCP - NCCAP & NAAPCC Certified Educator. The Course Provides all the CE Requirements for Path 1&2 - NAAPCC Standards Do you have 1 year of experience in the past 3yr working with the elderly as an assistant, a director or other? Do you have a high school diploma or higher? Do you hate doing practicum lessons about tasks you have been doing for years? Do you have 8 weeks to take the National Activity Professional Training (NAPT) Class and pass the National Board Certification Exam? Do you have the MEPAP1 Course? It is accepted at the NAAPCC. Do you have money and time to throw away? If not, then the NAAPCC Activity Board Certification Path is for you! One Class, One exam, One National Board Certification. NAAPCC "The Affordable Choice" Contact NAAPCC.Office@gmail.com Phone: 303-317-5682 Let their counselors reassure you you're on the right Path to National Board Certification. "Your Experience Counts!" See if you qualify! Check NAAPCC Standards The certifications recognized under CMS F Tag 680 for Activity Professionals are the NAAPCC AP-BC & AC-BC, NCCAP ADC & ACC, CTRS, OTR, and COTA. NAAPCC Est. 2011, is the only Activity Credentialing Organization that follows the ICE, NCCA Standards for Accreditation. They are NON-Profit. Contact NAAPCC.Office@gmail.com Phone: 303-317-5682 Let their counselors reassure you you're on the right Path to National Board Certification "Your Experience Counts!" See if you qualify! Check NAAPCC Standards American Healthcare Association's Shelter in Place: Planning Resource Guide for Nursing Homes Keep Residents, Staff and Family Members up to date with this blank Covid-19 Newsletter Template. Made simply for your convenience: Step 1: Click on Button below Step 2: Fill in sections with your info. Step 3: Hit print or email. Activity Directors Network was founded in 1996 on the idea that we could help create elderly care that dramatically improved the lives of those we all serve. We envision facilities that feel like homes and that celebrate our resident’s individuality and allows them to live with dignity, purpose and joy. We believe the exchange of education and wisdom between the most talented teachers and passionate students is the way to make an impact. Each and every single one of you are the revolution that is changing everything. Thanks for being a part of The Network. Copyright © 2020 Activity Directors Network, LLC All rights reserved. Our mailing address is: 2010 US HWY 190 W Ste 120 Livingston, Texas 77351